Retake
N31) Headache, vomiting, and difficulty with balance
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with headache.
- Review the DDx considerations in a patient with headache.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with headache.
History
A 35-year-old male presents to the emergency department with a two-week history of nausea, vomiting, headache, and blurry vision. The patient has also experienced difficulty with balance and coordination. The patient also has a history of a previously resected renal cell carcinoma and a family history of Von Hippel-Lindau disease.
Physical Exam
BP: 135/85, HR 86, RR 18, Temp 98.6, O2 saturation 95%. Neuro: dysmetria on finger-to-nose testing. There is papilledema. The patient loses balance with his feet together and eyes closed.
Labs
Labs are unremarkable aside from elevated hemoglobin indicating secondary polycythemia.
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient's symptoms of nausea, vomiting, headache, blurry vision, and papilledema suggest the presence of increased intracranial pressure. Furthermore, the patient's difficulty with balance and coordination, dysmetria, and positive Romberg's sign indicate cerebellar dysfunction. Given the patient's family history of VHL and previous history of renal cell carcinoma, there is a concern that the patient may have VHL syndrome. Therefore, it is likely that this presentation is secondary to obstructive hydrocephalus caused by an obstructing hemangioblastoma.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient with concern of an intracranial neoplasm and increased intracranial pressure requires urgent management.
First Imaging Study
What is the first imaging study you will order?
A head CT is an appropriate initial imaging modality as it can quickly and accurately identify the presence of a cerebral mass lesion and sequelae like hydrocephalus.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
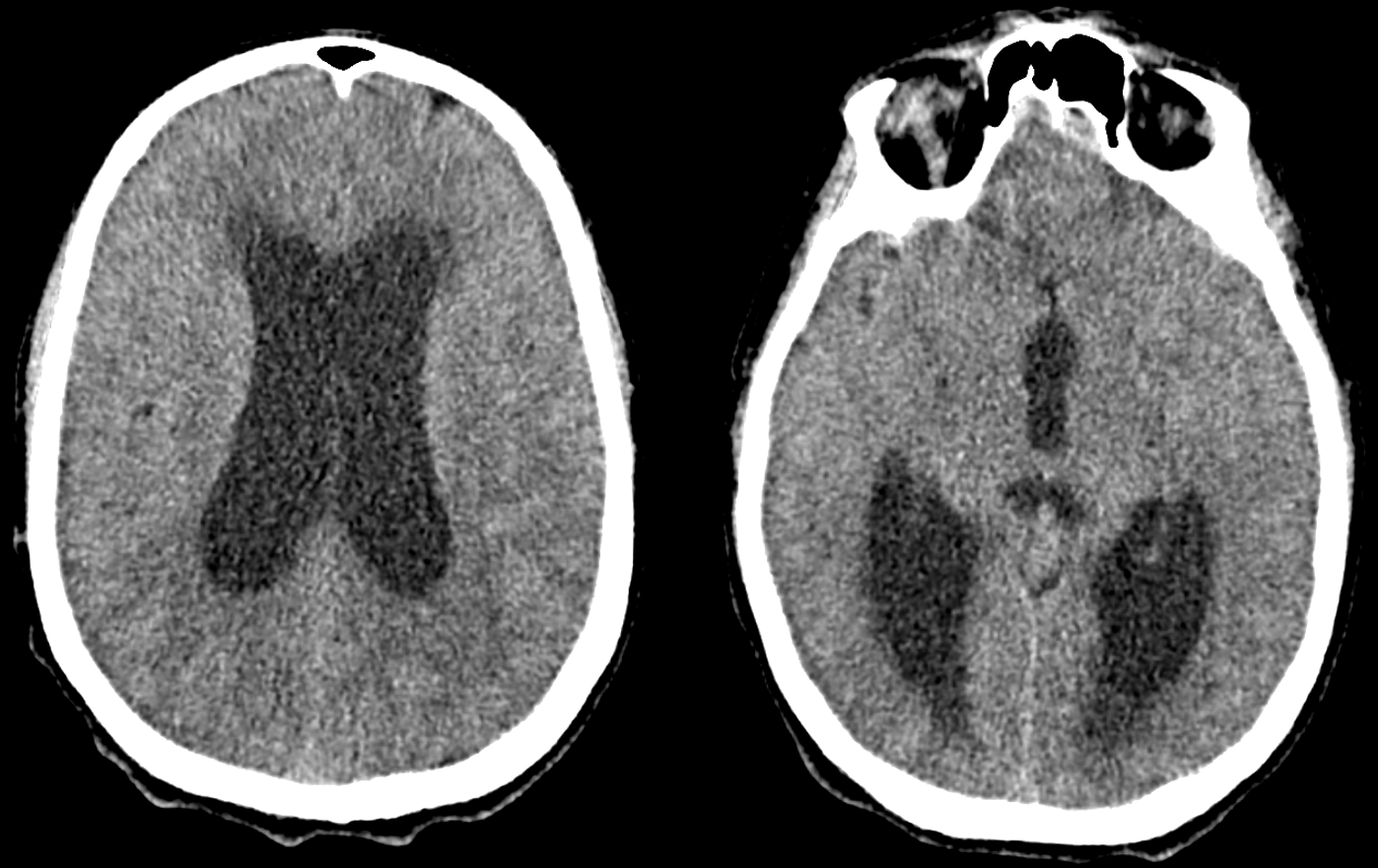
CT head
The ventricles are:
The lateral and third ventricles are significantly dilated, consistent with hydrocephalus.
There is a mass in the:
There is a mass in the infratentorial region in the brain.
What type of artifact is present?
There is beam hardening artifact, which occurs when X-rays pass through dense materials like metal, resulting in white streaks. In this case, the patient had right ear piercings. Motion artifact, caused by patient movement, would result in blurring, streaking, ghosting, or duplicate images. The patient’s ear piercings should be removed for any further imaging.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
An MRI may be performed to further characterize the lesion. Since hemangioblastomas are typically highly vascular lesions. MRI can also provide information about the vascular supply to tumor or complications not visible on the CT scan.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
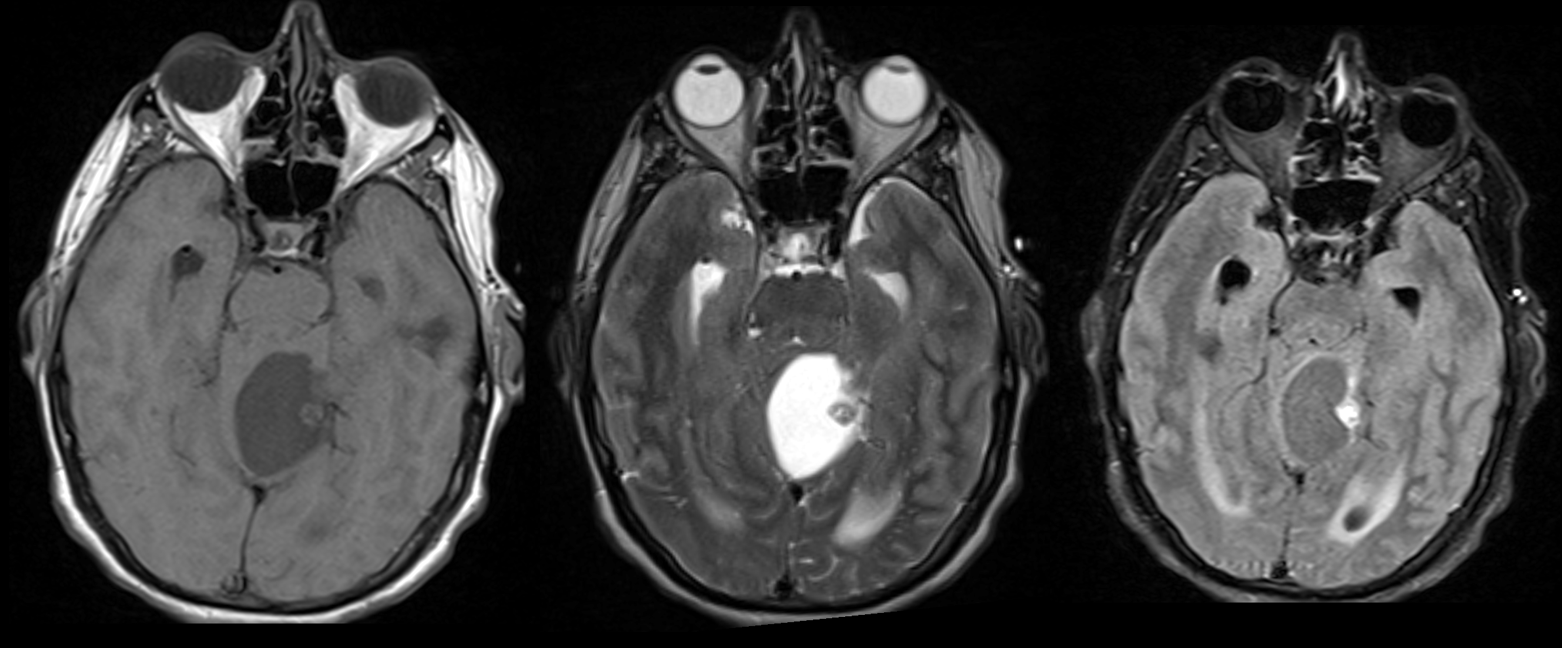
MRI head
The lesion is largely:
The lesion is most likely cystic and without significant proteinaceous material considering that there it is hypointense on T1 and hyperintense on T2.
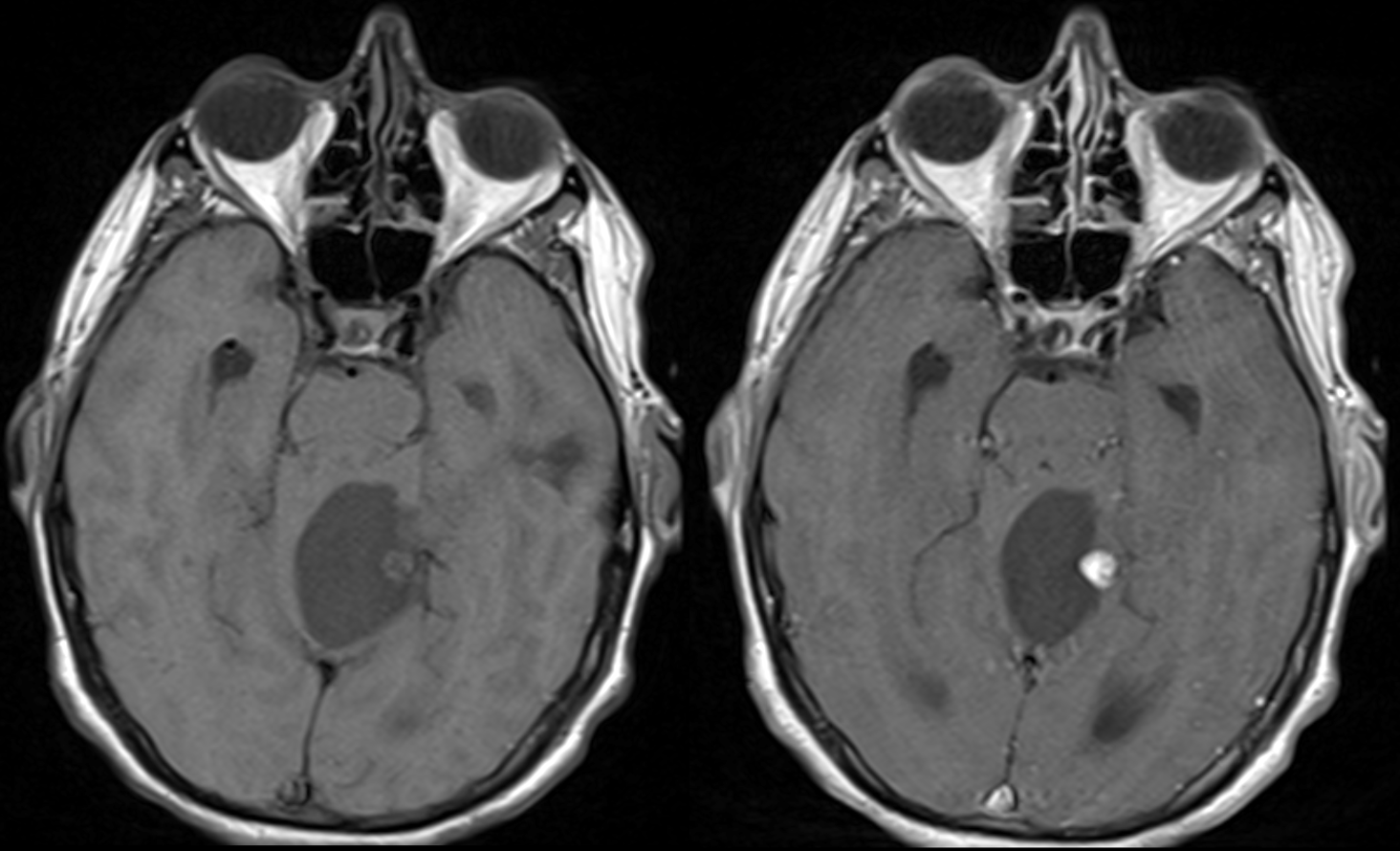
The mural nodule within the cystic lesion is enhancing.
The mural nodule vividly enhances after contrast is administered.
The mural nodule has:
The mural nodule of a hemangioblastoma is generally iso to hypointense on T1 and hyperintense on T2.
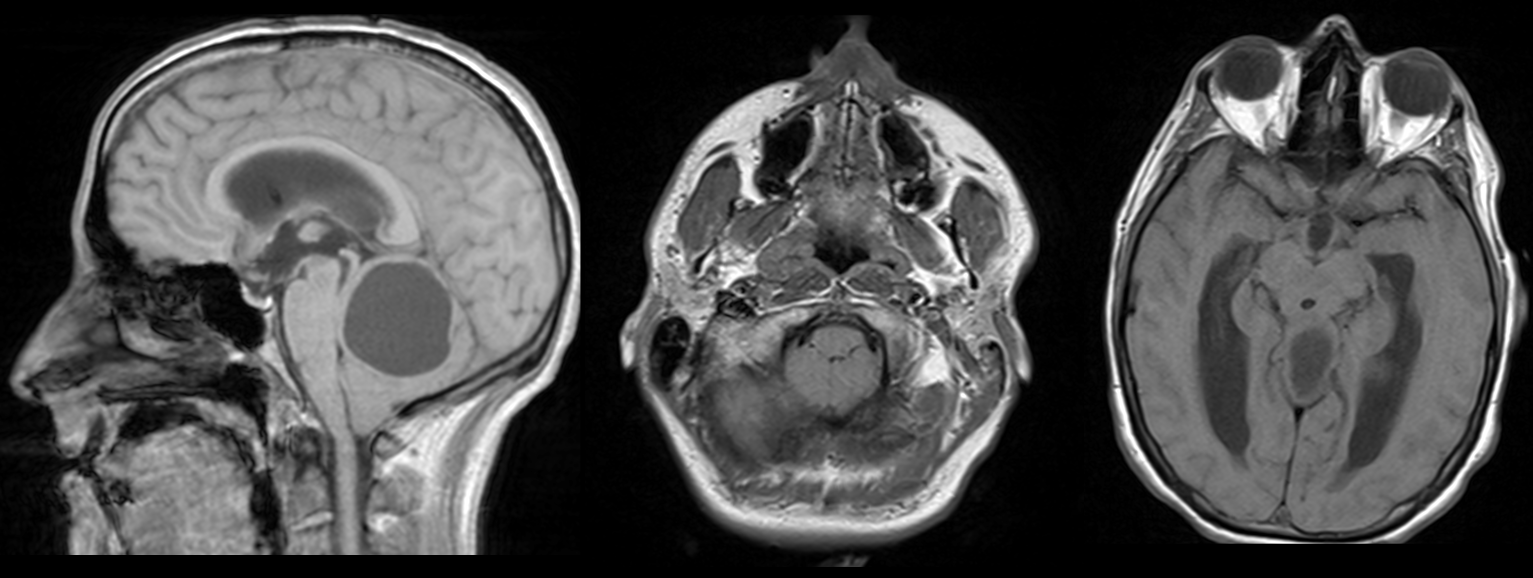
The upward transtentorial and downward tonsillar herniation has improved since the placement of an EVD.
There is a similar degree of upward transtentorial considering the obliteration of the cerebellar cisterns. There is also still downward tonsillar herniation considering the low-lying tonsils and crowding of the foramen magnum.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
No further imaging is required.
What is your Diagnosis now that you have seen the imaging results?
This with a family history of VHL and a past medical history of renal cell carcinoma now presenting with a hemangioblastoma likely has VHL.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This patient requires urgent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is a 35-year-old with a history of renal cell carcinoma and a family history of von Hippel-Lindau (VHL) disease who presents with symptoms of obstructive hydrocephalus due to a hemangioblastoma. Imaging studies show a cystic lesion with an enhancing mural nodule within the posterior fossa, causing significant mass effect with upward transtentorial herniation and downward tonsillar herniation. An external ventricular drain (EVD) was placed after the CT but did not alleviate the herniation. Neurosurgery should be contacted for urgent consideration of surgical intervention like a suboccipital craniotomy to reduce the mass effect and alleviate the herniation. The patient should also undergo frequent neurological examinations. Given the patient's history of renal cell carcinoma and family history of VHL disease, genetic testing should be considered to confirm the diagnosis.
Lessons Learned:
- Hemangioblastomas are typically benign tumors that most often occur in the cerebellum.
- Hemangioblastomas can occur sporadically or be associated with Von Hippel-Lindau Syndrome, a genetic disorder that predisposes individuals to the development of multiple tumors.
- A cerebellar hemangioblastoma is typically located within the posterior fossa and can be identified on CT or MRI as a cystic lesion with a vividly enhancing mural nodule. As these are highly vascular lesions, a flow void may sometimes be seen.
- If the hemangioblastoma is compressing the fourth ventricle, the patient may present with symptoms and signs of increased intracranial pressure secondary to obstructive hydrocephalus like nausea, vomiting, headaches, blurry vision, and papilledema. Imaging would reveal ventriculomegaly.
- Hemangioblastomas can also lead to intracranial hemorrhage and focal neurologic deficits due to compression of nearby CNS structures.
- The treatment of choice for hemangioblastoma is surgical resection, which has a relatively good prognosis with low recurrence rates.
Socioeconomic Factors: Positive prognostic factors in the overall survival for cerebellar hemangioblastoma include age less than 40, Caucasian race, female gender, and surgical intervention.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}